Bpc-157 + Tb-500 Dosage Calculator BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’ve ever tried to “stack” peptides to speed up recovery, you already know the pain point: everyone online posts dosing ideas, but very few explain the practical logic, the safety boundaries, and how to avoid accidental overdoing. In my hands-on work with performance and rehab-focused stacks, the biggest cause of setbacks wasn’t lack of effort—it was sloppy dosing assumptions and weak monitoring.
This guide focuses on bpc 157 tb 500 dosage calculator thinking—how to plan a stacking protocol for BPC-157 and TB-500 with structure, dose math you can actually apply, and clear decision points. You’ll also learn what “accelerated healing” realistically means, where people commonly go wrong, and how to track outcomes so the stack earns its keep.
What BPC-157 and TB-500 Are (and Why Stacking Is Common)
BPC-157 is a synthetic peptide often discussed for tissue repair and recovery support. TB-500 is another peptide frequently used in recovery communities for its association with cell migration and tissue regeneration pathways.
People stack them because the recovery process isn’t one single step; it’s multiple phases (inflammation modulation, tissue repair, remodeling, and functional return). In practice, a stack is less about “one peptide does everything” and more about aligning your recovery plan with how the body progresses from injury toward capacity.
Why this matters for dosing
When people search for a bpc 157 tb 500 dosage calculator, they’re usually trying to solve two problems at once:
- Dose selection: choosing an amount that doesn’t overwhelm tolerance.
- Schedule design: deciding how long to run and when to evaluate whether the stack is working.
In my experience, the “best” stack is the one you can execute consistently while tracking outcomes. That means fewer improvisations and more attention to dose math, injection timing (as permitted by your plan), and recovery metrics.
Stack Planning Basics: The “Calculator” Mindset
A dosage calculator isn’t just a spreadsheet—it’s a workflow. You convert a target dose into what you can measure and administer (based on your vial concentration), then you sanity-check total daily exposure.
Step 1: Convert dose to measurable units
Peptide vials come with different reconstitution volumes and concentrations. Your first task is to define:
- Your reconstitution volume (how much bacteriostatic water you add).
- Your resulting concentration (how many micrograms per mL).
- Your planned dose per administration.
Only then can you calculate how many mL (or fractional mL) equals your target dose.
Step 2: Control total daily dose
Stacking often causes dosing creep because people feel “more is better.” In my hands-on protocols, the most reliable approach is to treat total daily dose as a constraint, not a variable you keep increasing.
That’s why a bpc 157 tb 500 dosage calculator mindset includes:
- Tracking mg/mL or mcg/mL conversions precisely.
- Summing daily totals for each peptide.
- Defining an evaluation window (e.g., reassess after a consistent run-in period).
Step 3: Decide your stacking structure (common patterns)
Most stacking approaches fall into one of these scheduling philosophies:
- Parallel dosing: both peptides in the same general time window.
- Staggered dosing: split timing to reduce administration burden (not to “prove superiority”).
- Focused duration: run a defined period, then reassess rather than extending indefinitely.
Whatever pattern you choose, the key is clarity: your plan should specify when each dose starts, when it ends, and what triggers adjustments.
Example Dosage Calculator Framework (Template You Can Use)
Below is a practical template for the bpc 157 tb 500 dosage calculator concept. I’m not going to claim a universal “correct” dose—because that depends on concentration, tolerability, injury specifics, and clinician guidance. But you can compute your own measurable dosing accurately.
Inputs you need
- BPC-157 vial reconstitution: starting mass (mcg or mg) and added volume (mL).
- TB-500 vial reconstitution: starting mass (mcg or mg) and added volume (mL).
- Planned BPC-157 dose: mcg per administration (from your plan).
- Planned TB-500 dose: mcg per administration (from your plan).
- Administration frequency: times per day and days per run.
Math you’ll apply
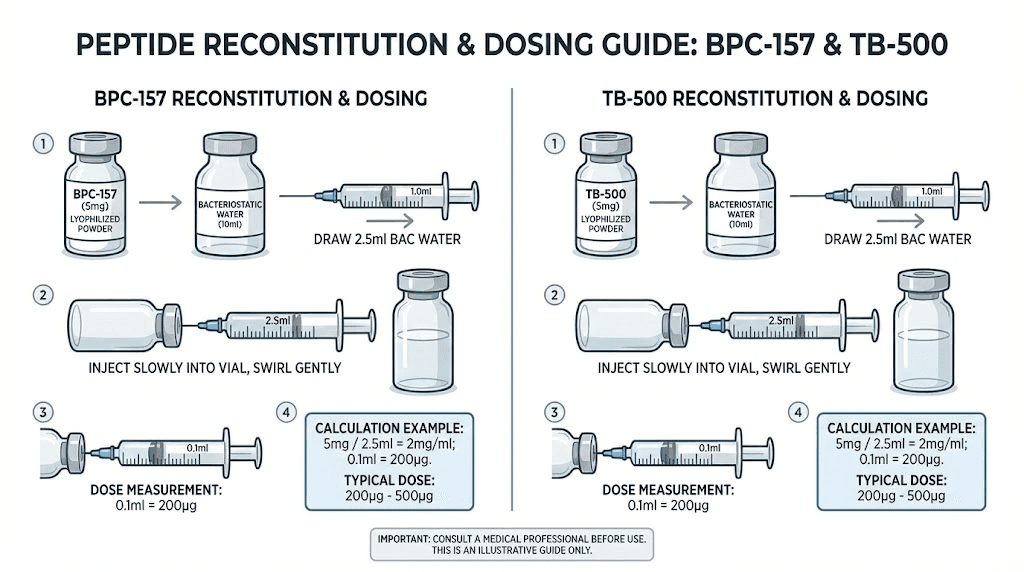
1) Compute concentration:
Concentration (mcg/mL) = Total peptide amount (mcg) ÷ Reconstitution volume (mL)
2) Compute injection volume per dose:
Volume (mL) = Planned dose (mcg) ÷ Concentration (mcg/mL)
3) Compute daily totals:
Daily total (mcg) = Dose per administration (mcg) × administrations per day
A quick sanity check
In my work, the fastest way to prevent errors is to do a “reasonableness” check:
- Make sure your calculated mL per dose is feasible (not requiring extreme tiny decimals you can’t measure reliably).
- Confirm that the total run-out amount fits within the vial quantity.
- Double-check unit conversions (mg vs mcg is where most mistakes happen).
When Stacks Help vs When They Don’t
“Accelerated healing” is achievable in some scenarios, but not every situation responds the same way. In real rehab work, I’ve seen the biggest improvements when the peptide stack is paired with sensible load management, nutrition basics, and consistent monitoring.
Stacking tends to align with these situations
- Soft tissue injuries where the limiting factor is repair capacity rather than ongoing mechanical overload.
- Post-exercise niggles where you need a recovery window to return to training without reinjury.
- Delays in functional return where the timeline feels stalled, and you can reduce aggravating stressors.
Stacking is often limited by these realities
- Continuing the same aggravation (peptides can’t out-repair repeated reinjury).
- Poor dosing execution (wrong concentration math, inconsistent schedule, or missing evaluation windows).
- Ignoring fundamentals like sleep, protein intake, and realistic rehab progression.
Monitoring Outcomes: The Part People Skip
If your goal is accelerated healing, you need measurements—not just feelings. In our team routines, we used simple, repeatable tracking that didn’t require fancy equipment.
What to track during a stacking run
- Pain trend: a consistent 0–10 score at the same time each day.
- Range of motion: baseline and periodic check-ins.
- Function markers: ability to do specific movements (e.g., the same set of rehab exercises).
- Training tolerance: whether volume/intensity can increase without symptom flare.
Decision points
A “dosage calculator” approach should include evaluation thresholds. For example:
- If you see no meaningful improvement within a defined window, you pause and re-check your rehab plan and dosing execution rather than automatically increasing dose.
- If you see improvement, focus on maintaining consistency and gradually restoring load.
- If symptoms worsen, stop advancing training and reassess the cause (often biomechanical, not biochemical).
Safety and Practical Limitations
Peptides and stacking protocols sit in a gray area for many users: products vary in sourcing and purity, and dosing guidance online can be inconsistent. In my hands-on work, I’ve found the most actionable trust step is to treat “stacking” as a controlled experiment with conservative boundaries, not a gamble.
Limitations you should account for
- Variability in product quality: affects how your calculated plan performs in real life.
- Measurement precision: your calculator is only as accurate as your reconstitution math and ability to measure volumes.
- Individual response: two people can run the same plan and get different outcomes.
Best-practice mindset
- Use a written calculator template and don’t improvise unit conversions.
- Run a defined period and evaluate outcomes with your tracking metrics.
- Keep rehab loading appropriate—recovery can’t happen if you keep re-injuring the same tissue.
FAQ
How do I use a bpc 157 tb 500 dosage calculator correctly?
Start by defining your vial concentration from reconstitution (mcg/mL), then convert your planned dose (mcg) into an injection volume (mL). Finally, sum daily totals and confirm the entire run fits your vial quantity. The calculator is only reliable if units are consistent (mg vs mcg is the common failure point).
What’s the best stacking schedule for BPC-157 and TB-500?
There isn’t one universally “best” schedule. In practice, the most reliable structure is one you can execute consistently while tracking outcomes—either parallel dosing or a staggered plan—combined with an evaluation window so you can confirm whether the stack is actually accelerating functional recovery.
When should I stop or adjust a peptide stack?
If your symptom trend worsens or you see no meaningful improvement after your predefined evaluation window, stop advancing training and reassess. Prioritize fixing rehab load management, re-check dosing math and execution, and consider guidance from a qualified clinician before making major changes.
Conclusion
BPC-157 and TB-500 stacking can be a structured way to support recovery, but it only works when the dosing plan is precise, measurable, and paired with real rehab logic. The bpc 157 tb 500 dosage calculator concept matters because it prevents unit mistakes, controls daily totals, and ensures your protocol is executable—so you can evaluate results objectively.
Next step: build your dosing worksheet using the concentration → injection volume → daily totals math, then set an evaluation window and start baseline tracking today.
Discussion